Otitis Media with Effusion – October 17, 2024
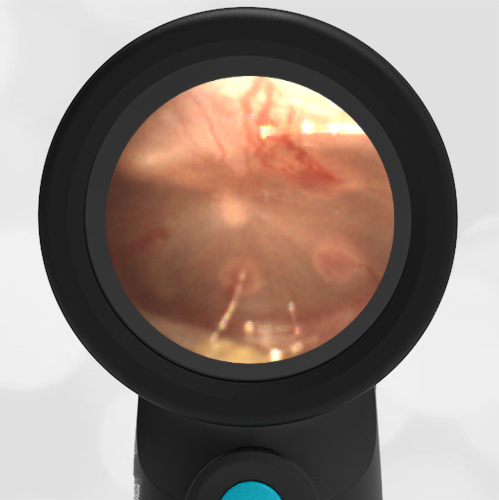
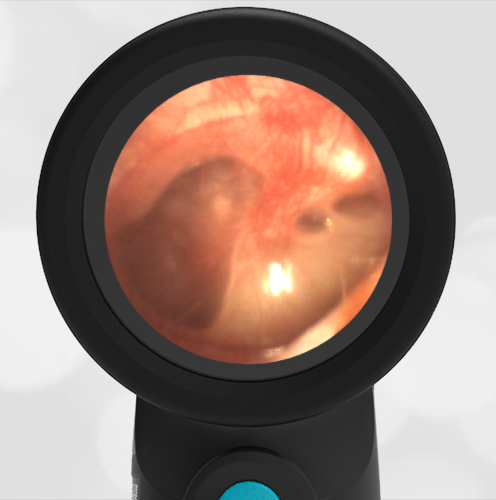
A 12-month-old female presented to the pediatric emergency department (ED) with concern for an ear infection. The mother reported a week of runny nose and mild cough as well as subjective fever. The day prior, she was putting a finger into her right ear, so she was taken to Urgent Care where she was diagnosed with an ear infection. The mother reported the child was refusing to take the “pink antibiotic”, so they came to the ED seeking an alternative. Upon evaluation, the child is afebrile with normal vital signs. She has clear nasal drainage. Auscultation revealed very mild wheezes bilaterally. The Wispr digital otoscope exam is attached below.
What is the appropriate management for this child’s condition?
- Discontinue the antibiotic and recommend supportive measures
- Continue the current antibiotic, but recommend putting it in juice or syrup to mask the taste
- Change the antibiotic to amoxicillin plus clavulanate
- Refer the child to otolaryngology (ENT) for audiometry and tympanostomy tube placement
Answer: A. Discontinue the antibiotic and recommend supportive measures

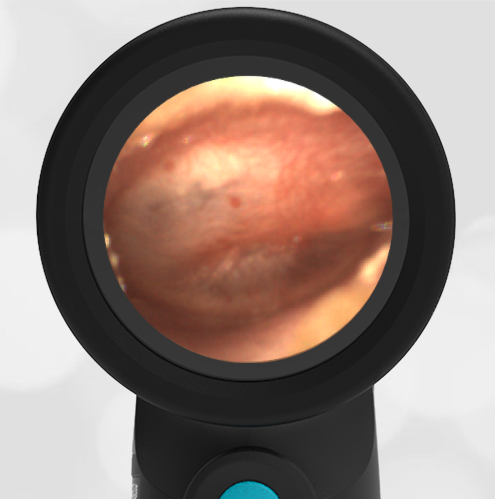
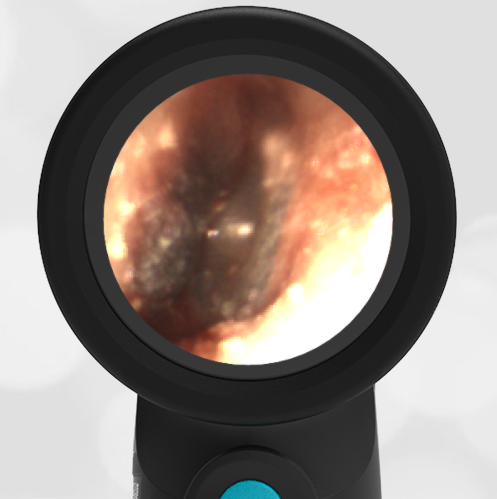
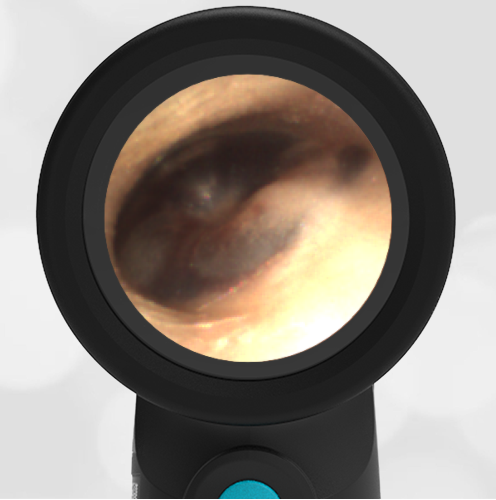
This child’s Wispr otoscope exam demonstrates a right-sided middle ear effusion (MEE) as evidenced by visible air bubbles behind a clear tympanic membrane (TM, “ear drum”). Since the child’s TM is not bulging (notice how the malleus is easily identified) nor is there marked erythema (redness), the diagnosis of Acute Otitis Media (AOM) should not be made. Therefore, her diagnosis is most consistent with Otitis Media with Effusion (OME) which does not require treatment with antibiotics. The presence of the air-fluid levels without bulging indicates that the Eustachian tube is ventilating the middle ear space appropriately.
OME is a common finding in young children with viral respiratory infections that may occur following a bout of AOM or simply because of Eustachian tube dysfunction. In both instances, the child may exhibit signs of discomfort that may incline one to overtreat as presumed AOM if the diagnosis is not certain. This case reinforces the importance of adequate visualization of the TM to avoid this pitfall. Beyond symptomatic management, referral to ENT for evaluation may be indicated if the child has risk factors for hearing loss (such as craniofacial abnormalities, known hearing deficits, or language delays) or if the OME persists beyond three months.
WiscMed has created a visual guide to common ear conditions that may be found here.
Key Learning Points
-Proper visualization of the tympanic membrane is required for any diagnosis
–Otitis Media with Effusion is characterized by air-fluid levels behind the tympanic membrane without evidence of bulging or loss of bony landmarks.
–Otitis Media with Effusion does not require antibiotics
Here is the complete video exam
Reference: