Diagnosis Guides
Diagnosis Guides



Acute Otitis Media (AOM) develops over time. Medical history typically includes a prodrome of viral symptoms such as fever, cough, rhinorrhea and congestion. Often, ear pain will start about 3 days after the onset of the prodrome symptoms. The mechanism is generally thought to be inflammation in the middle ear space from the viral infection. This often leads to Eustachian tube dysfunction. The "noodle like" portion of the Eustachian tube becomes inflamed and essentially clogged. The middle ear space can no longer drain via the Eustachian tube. Pressure builds in the middle ear space between the tympanic membrane and the clogged Eustachian tube causing bulging of the tympanic membrane and pain. Because the middle ear space is poorly draining and poorly ventilated, an opportunity for bacterial co-infection occurs.
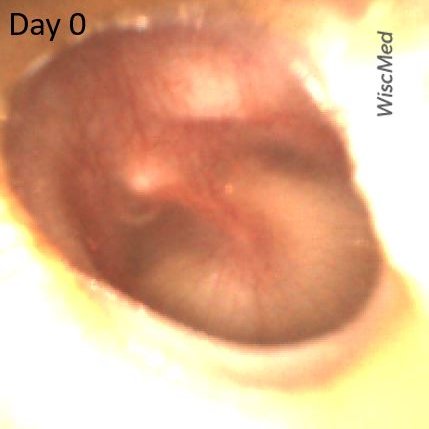
An 18-month-old female is brought into the emergency department (ED) with concerns for vomiting, fever, and fussiness. The child had historically been well and is age-appropriate vaccinated. The symptoms began 2 days earlier. Symptoms initially included pulling at the ears, escalating to vomiting, poor feeding, and fever to 103 F. The parents treated with antipyretics but became concerned when the child seemed to be declining further. They brought her to the ED with a primary concern of dehydration. In the ED, she was found to have a brisk capillary refill, elevated heart rate and a fever of 102 F. Influenza and COVID tests were both negative. Urinalysis was also negative. The following image of her left ear was obtained. Would you start the child on antibiotics based on the history, exam, and imaging presented?

Left ear day 0 exam - does not meet criteria for AOM
This is a typical case seen in the pediatric emergency department. A previously well child with signs and symptoms often associated with a common and benign viral infection. The pressing issue is to rule out treatable conditions. In a female child this age, those conditions would commonly be a urinary tract infection (UTI) or acute otitis media (AOM). As noted, she did not have a UTI on urinalysis.
Given the image found on Wispr otoscopy, the question of treatment for AOM is not straightforward. The left ear is clearly not normal. There is evidence of purulence in the middle ear space and the pars flaccida portion of the tympanic membrane (TM) is bulging. However, the malleus ossicle is still discernable, and the bulging of the pars tensa portion of the TM is minimal. In addition, there is an air-fluid bubble present indicating that the Eustachian tube is still functioning and suggesting a middle ear effusion (MEE).
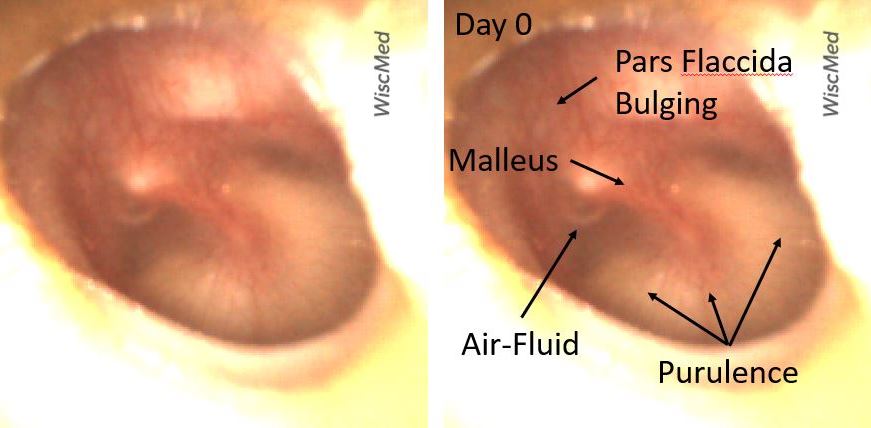
Left ear day 0 exam annotated - does not meet criteria for AOM
In consultation with the mother, the decision was made not to start antibiotics for AOM at this time. The patient was re-presented to the pediatric clinic the next day as symptoms did not improve. The following image was obtained on the next-day visit:

Left ear day 1 exam - Meets criteria for AOM
On this serial exam, the disease process in the ear has progressed. The bulging of the entire eardrum is significant indicating increased pressure in the middle ear space and a poorly functioning Eustachian tube. There is increased purulence behind the tympanic membrane. A small air-fluid bubble is still visible, likely air trapped previously and not an indication of a properly functioning Eustachian tube.

Left ear day 1 exam annotated - meets criteria for AOM
With these findings, the child was placed on an antibiotic. She had rapid improvement in her symptoms within a day. This case shows the importance of careful consultation with family members about the natural history of disease and strong encouragement to return for evaluation if symptoms worsen.
Here are the day 0 and day 1 video exams:
Left Ear - Day 0
Left Ear - Day 1