Otitis Media with Effusion – August 17, 2023
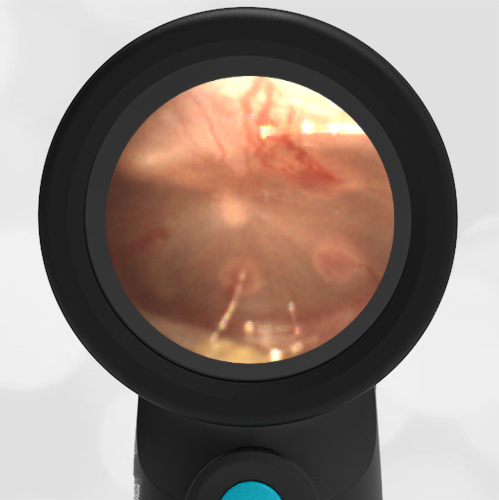
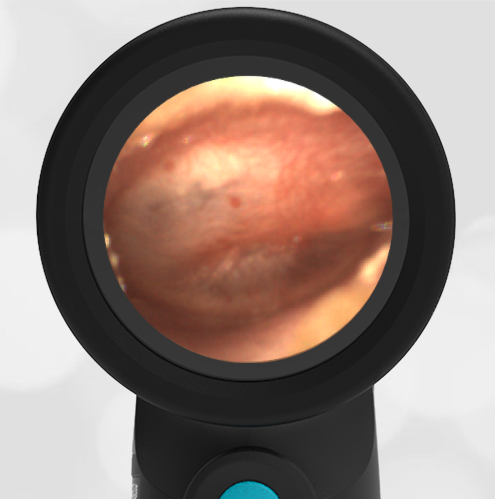
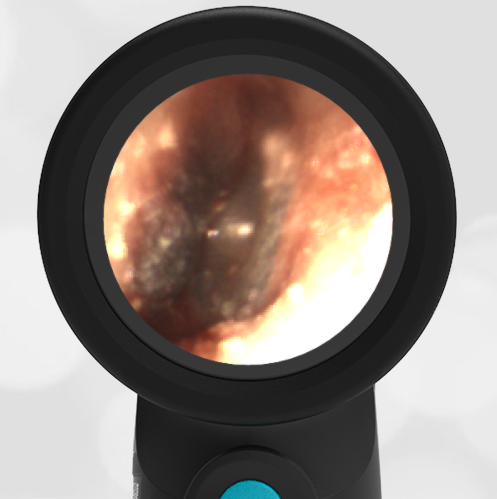
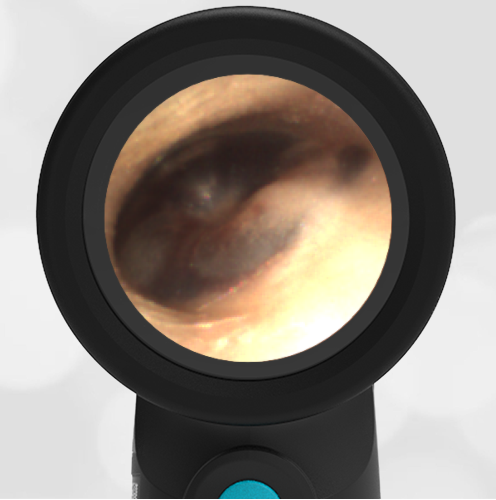
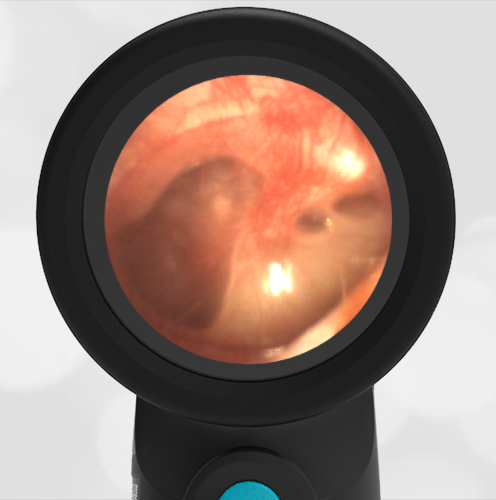
A 2-year-old presents to the emergency department (ED) for evaluation of ear discomfort after his mom noticed him sticking his finger into his right ear. The mom states the child has had several ear infections, the most recent infection being 2 months ago that was treated with antibiotics. Mom reports some concern about his hearing—she notes her son puts his fingers in his ears “a lot” and is lagging behind in his expressive language development. The child has nasal congestion and a low-grade fever but is otherwise well-appearing. The WiscMed Wispr digital otoscope exam is shown.
Which of the following is the most appropriate course of action now?
- The ear is normal, no management is necessary.
- Antibiotics should be prescribed.
- Refer the child to otolaryngology (ENT) for tympanostomy tubes.
- Provide symptomatic relief suggestions and have the child follow up with his pediatrician.
Answer: D. Provide symptomatic relief suggestions and have the child follow up with his pediatrician.
This child has Otitis Media with Effusion (OME) which is defined as middle ear effusion (MEE) without signs of infection of the fluid or inflammation of the tympanic membrane (TM). The hallmarks of OME are air-fluid levels behind a tympanic membrane that is not bulging. Because the TM is not bulging, the malleus ossicle is clearly distinguishable. The fluid is located in the middle-ear space. The lack of bulging and the presence of air along with the fluid suggests that the Eustachian tube is functioning properly.

OME most often occurs as a result of resolving AOM or in association with a viral upper respiratory infection. While typically requiring only supportive care, it should be noted that OME is also at the intersection between resolving AOM, evolving AOM, or Chronic Otitis Media with Effusion (COME), see Diagram 1.

Diagram 1: Relationship of middle ear findings
WiscMed has created a visual ear diagnosis guide that may be found here.
Given mom’s concerns about her child’s hearing, follow-up with the pediatrician is prudent to ensure the fluid does not persist. Current recommendations for ENT referral and consideration for tympanostomy tubes depend on a number of factors including age of the child, duration of MEE, and number of confirmed cases of AOM. The most recent American Academy of Otolaryngology-Head and Neck Surgery guidelines published in 2013 recommend tympanostomy tube (TT) placement for:
1. Bilateral chronic otitis media with effusion (OME) for three months or longer AND documented hearing loss.
2. Unilateral or bilateral OME for three months or longer AND reduced quality of life, ear discomfort, poor school performance, behavioral problems, vestibular problems, or other symptoms that could be attributable to OME.
3. Recurrent acute otitis media (RAOM), defined as three episodes of AOM in 6 months or four episodes in 12 months treated with antibiotics, WITH unilateral or bilateral middle ear effusion at the time of assessment for tube candidacy.
4. At-risk children with unilateral or bilateral OME, which is unlikely to resolve quickly for three months or longer. At-risk children are defined as those with permanent hearing loss independent of OME, speech and language delay, developmental disorders including autism, syndromes or craniofacial disorders which include cognitive, speech, or language delays, blindness or an uncorrectable visual impairment, cleft palate, or developmental delay.
Here is the complete video exam.
Reference:
Rosenfeld RM, Schwartz SR, Pynnonen MA, et al. Clinical Practice Guideline: Tympanostomy Tubes in Children. Otolaryngology–Head and Neck Surgery. 2013;149(1_suppl):S1-S35. doi:10.1177/0194599813487302