Resistant Acute Otitis Media – April 25, 2024
A three-year-old male presents to the emergency department (ED) for “medication management” after a recent diagnosis of acute otitis media (AOM). His family reports the child has had multiple bouts of AOM with his most recent diagnosis three days ago. Two weeks prior, he was treated for his fourth AOM in five months. He completed a course of antibiotics without difficulty, however, he continued to stick his finger in his ears and seemed uncomfortable. The parents had their child re-evaluated and bilateral AOM was noted. A discussion of prior management revealed he had been treated with four different antibiotics. He has an appointment with ENT in three months, the earliest he could get in. At the time of his current diagnosis, a plan for three days of intramuscular (IM) antibiotics was agreed upon. He received his first two doses without difficulty and presented to the ED for his third dose due to the schedule falling on a weekend. Of note, the family was turned away from an Urgent Care who refused to administer “too much” ceftriaxone. His Wispr digital otoscope exam from his current visit is shown.
Which of the following is correct regarding this child’s presentation?
- His initial diagnosis of AOM is incorrect and he does not require an intramuscular antibiotic.
- His initial diagnosis of AOM is correct but he should be treated with an oral antibiotic.
- His current exam demonstrates persistent AOM and referral for immediate tympanostomy (ear tubes) is indicated.
- His current exam indicates improvement and continued treatment with 3rd dose of intramuscular antibiotic is appropriate.
Answer: D. His current exam indicates improvement and continued treatment with 3rd dose of intramuscular antibiotic is appropriate.
-

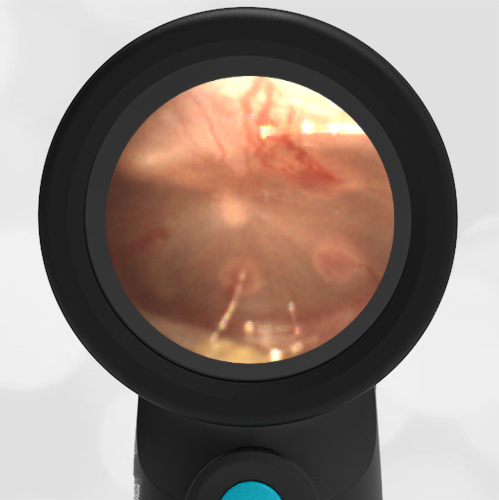
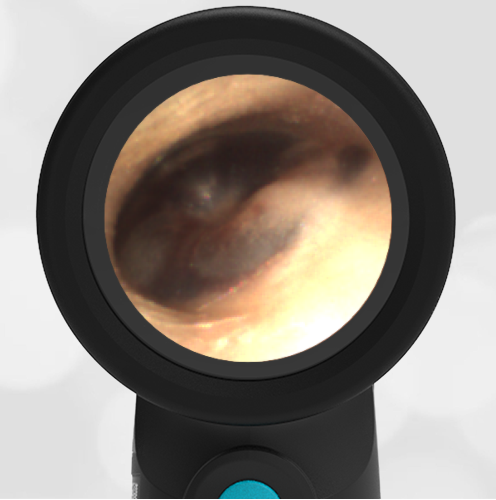
- Initial AOM
-
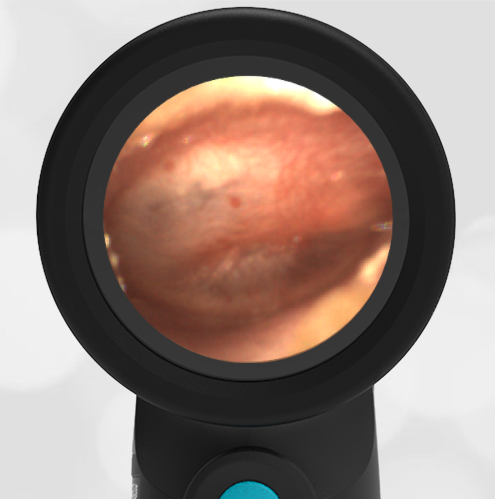
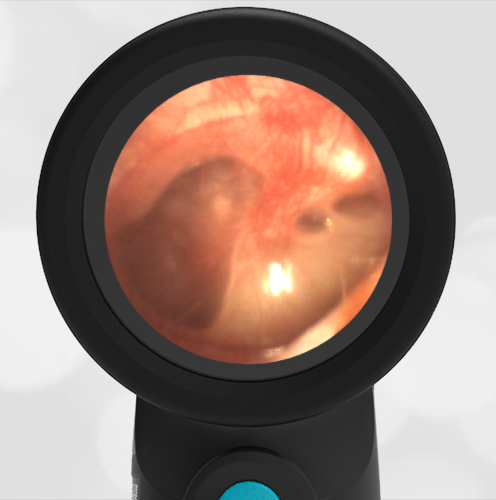
- Improving AOM
The child’s initial Wispr exam demonstrates AOM as evidenced by severe bulging. His repeat exam following the two doses of IM antibiotics demonstrates improvement with significantly less bulging.
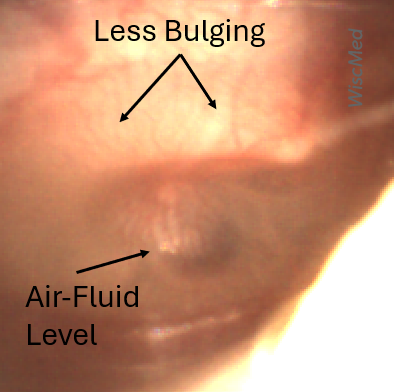
He continues to have a cloudy middle ear effusion (MEE), but this would be expected only two days into treatment. The air-fluid level suggests that the Eustachian tube is now venting the middle ear space. Given the improvement, there is no current indication for ear tubes. While single dose IM ceftriaxone is an acceptable option for children who do not tolerate oral medications, it may not be sufficient in children with multiple treatment failures. Therefore, given his history of difficult-to-clear AOM, continued treatment with the third dose of IM antibiotics is appropriate.
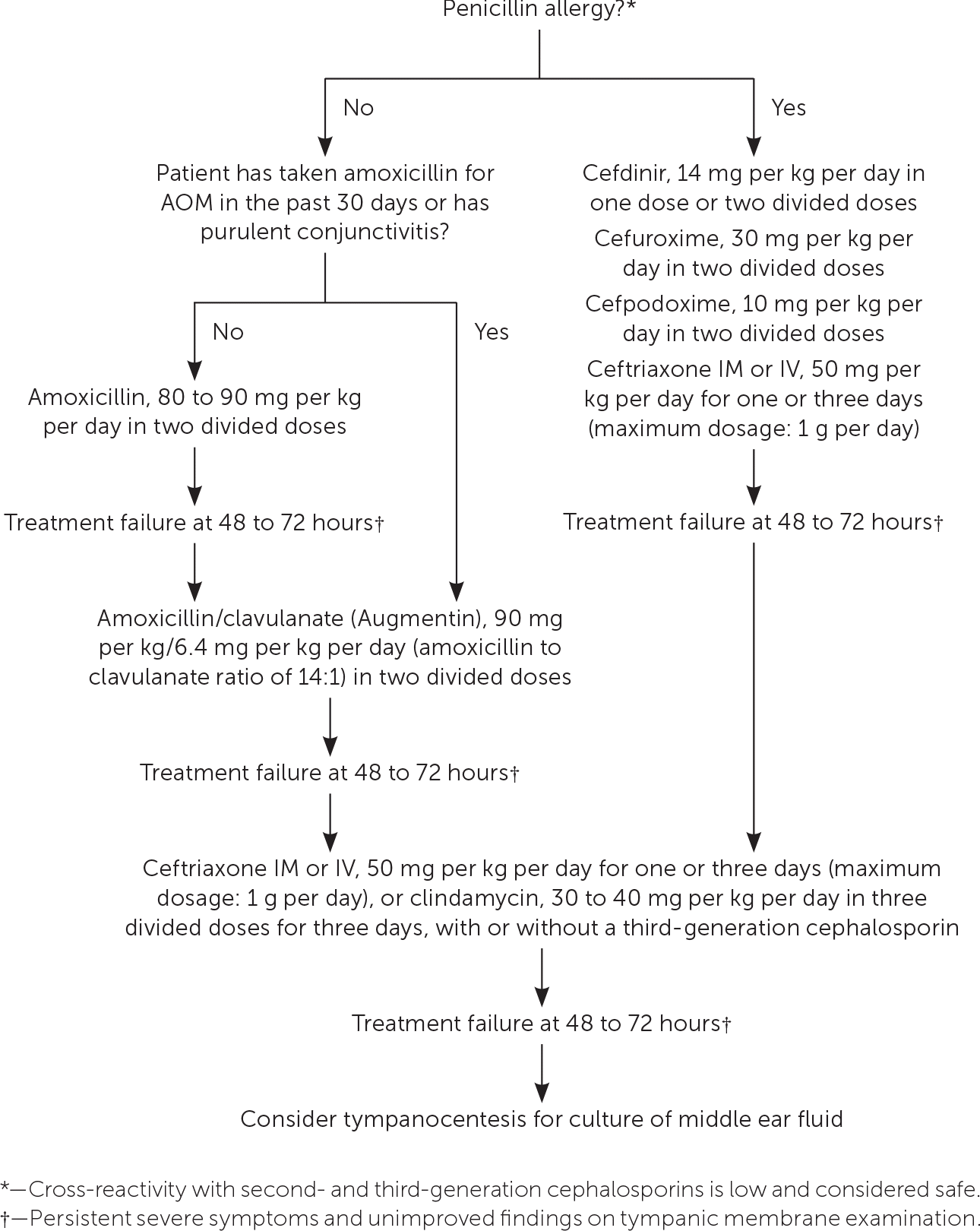
While treatment strategies will continue to evolve, the following diagram from aafp.org utilizes the 2013 AOM Practice Parameter:
References:
Leibovitz E, Piglansky L, Raiz S, Press J,Leiberman A, Dagan R. Bacteriologic and clinical efficacy of one day vs. three-day intramuscular ceftriaxone for treatment of nonresponsive acute otitis media in children. Pediatr Infect Dis J. 2000;19(11):1040–1045.
Lieberthal AS, Carroll AE, Chonmaitree T, Ganiats TG, Hoberman A, Jackson MA, Joffe MD, Miller DT, Rosenfeld RM, Sevilla XD, Schwartz RH, Thomas PA, Tunkel DE. The diagnosis and management of acute otitis media. Pediatrics. 2013 Mar;131(3):e964-99. doi: 10.1542/peds.2012-3488. Epub 2013 Feb 25. Erratum in: Pediatrics. 2014 Feb;133(2):346. Dosage error in article text. PMID: 23439909.
Here is the complete video exam